Do you have a “quotation that inspires you”? The one I would choose is probably not an obvious one for a health blog. You might have been expecting me to have trawled through the “inspirational” websites to find some relevant, life affirming words. I hope you’re not disappointed….
Here goes. Over to that well known, now deceased, US philosopher, Donald Rumsfeld. It’s the quote he was ridiculed for at the time, unfairly in my opinion, as it makes perfect sense. In case you don’t remember what he said : “…as we know, there are known knowns; there are things we know we know. We also know there are known unknowns; that is to say we know there are some things we do not know. But there are also unknown unknowns- the ones we don’t know we don’t know.”
Bear with me, I hope it will become clear. To illustrate the point I’m using a subject I feel particularly strongly about – bile acid malabsorption (BAM). As someone actively engaged in research into bowel issues, I’ve read many comments from patients who have recently been diagnosed with BAM and many times they go on to say that their doctor had never heard of the condition before. That’s the first hurdle to overcome.
Using my limited AI skills I asked ChatGPT to draw this image. I posted it on various FB forums and the responnse we saddening as so many sufferers
If you have been diagnosed with BAM you’ll know that it causes chronic diarrhoea. Bile acid is usually recirculated to the gallbladder via the far end of the small intestine. If that area is damaged or compromised the bile acid passes directly into the colon triggering the secretion of extra water, leading to looser stools. It can be a very debilitating condition.
I am a fellow sufferer as a result of losing my terminal ileum. (I had an ileostomy back in October 2010. Full story in my book! Before the operation I was offered the chance to take part in an Enhanced Recovery Scheme at one of the top London hospitals. Part of the ethos behind this regime is to fully inform the patient of what will happen at all stages of the process – pre-op, during the hospital stay and beyond. Was I told about BAM before the operation? I’d have to answer “maybe” and this brings us to the point of this post. Let me explain….
I was expecting my digestive system to function normally after the surgery. The Enhanced Recovery Nurse and the surgeon had told me that absorption of vitamins and salts would be much reduced as I would no longer have a terminal ileum. If someone told you that your body wouldn’t absorb salts properly what would you take that to mean? I took it at face value, I would need to up my intake of salt (sodium chloride) to compensate and take supplemental vitamins. I didn’t see the need to question the statement as it seemed very clear. Maybe I should have been more curious as I left hospital with a long term prescription for 12 Imodium capsules per day.
In fact it took four years before I underwent a SeHCAT scan and was diagnosed with severe BAM. It was then that I discovered it has an alternative name “Bile SALT Malabsorption”. Suddenly the comment about not absorbing “salt” took on another meaning. You can see the problem.
This is where Donald Rumsfeld comes in. I heard what the Enhanced Recovery Nurse and the surgeon told me; I understood what the words meant to me; but didn’t appreciate what the words meant to them. From their point of view – they were using their everyday, medical terms to describe a likely problem to a patient. From this experience I have learnt to always question what I am being told and to do my best to get the doctor, consultant or surgeon to explain, in simple or non-medical terms, exactly what they mean and what they perceive the implications to be.
I keep coming back to those particular words in the quote “there are things we don’t know we don’t know.” Try repeating them to yourself as you enter the consulting room…..
Using my limited AI skills I asked ChatGPT to draw this image. I posted it on various FB forums and many of the responses were saddening as so many patients had suffered from this debilitating condition for years, undiagnosed, and it had badly affected their QOL.
In 2025, as part of the “Wrestling The Octopus – The IBD Patient Podcast”, we interviewed one of the UK’s leading experts on bile acid malabsorption, Prof. Julian Walters. If you want to know more about the condition this give this episode a listen.
If you’re about to have your first video capsule endoscopy (VCE) or simply wondering what the experience is like then read on. I underwent my third procedure in September 2023, each one has been slightly different.
Fantastic Voyage – revisited
In November 2018 I had my first VCE and afterwards published a blog post “Fantastic Voyage” as it reminded me of that sci-fi film about a submarine crew who are shrunk to microscopic size and venture into a body to repair a damaged organ. What follows updates that post and then goes on to describe the two further procedures.
Why did I need a VCE in the first place?
I was feeling fit, well and with a good QOL. Colonoscopies, endoscopies & biopsies were all clear but… test results were suggesting the opposite – calprotectin approaching 2000 (normal range 50 to 100); Hb hovering around 110 (not particularly low but on the way down); and I was losing weight (down by 15kg). The only part of my digestive tract that hadn’t been seen through a lens was the small bowel between duodenum and my anastomosis, where my large and small intestines had been rejoined after an ileostomy in 2010.
With a capsule there is always a risk of it becoming stuck so as a precaution a radiologist was asked to review my last MRI scan for strictures before the VCE was ordered. The alternative is to swallow a patency capsule which is a dissolvable pill that surrounds a small radio frequency identification (RFID) tag that can be identified by an X-ray or CT scan. If the pill become lodged in the gut it simply dissolves. The latest cost (2025) that I could find for an NHS capsule endoscopy procedure is £747.
The pre-procedure instructions were similar to having a colonoscopy but with none of the dreaded prep solution. The leaflet listed the medications that would have to be put on hold. These included iron tablets and loperamide 7 days out. Iron tablets – no problem, but loperamide – that was one instruction I didn’t follow. The thought of taking a trip to London without having taken it for 7 days was not even worth considering.
On arrival at the GSTT Endoscopy Department a specialist nurse outlined the procedure and ran through the risks. In the worst case scenario the capsule could become stuck and need surgery to recover it!
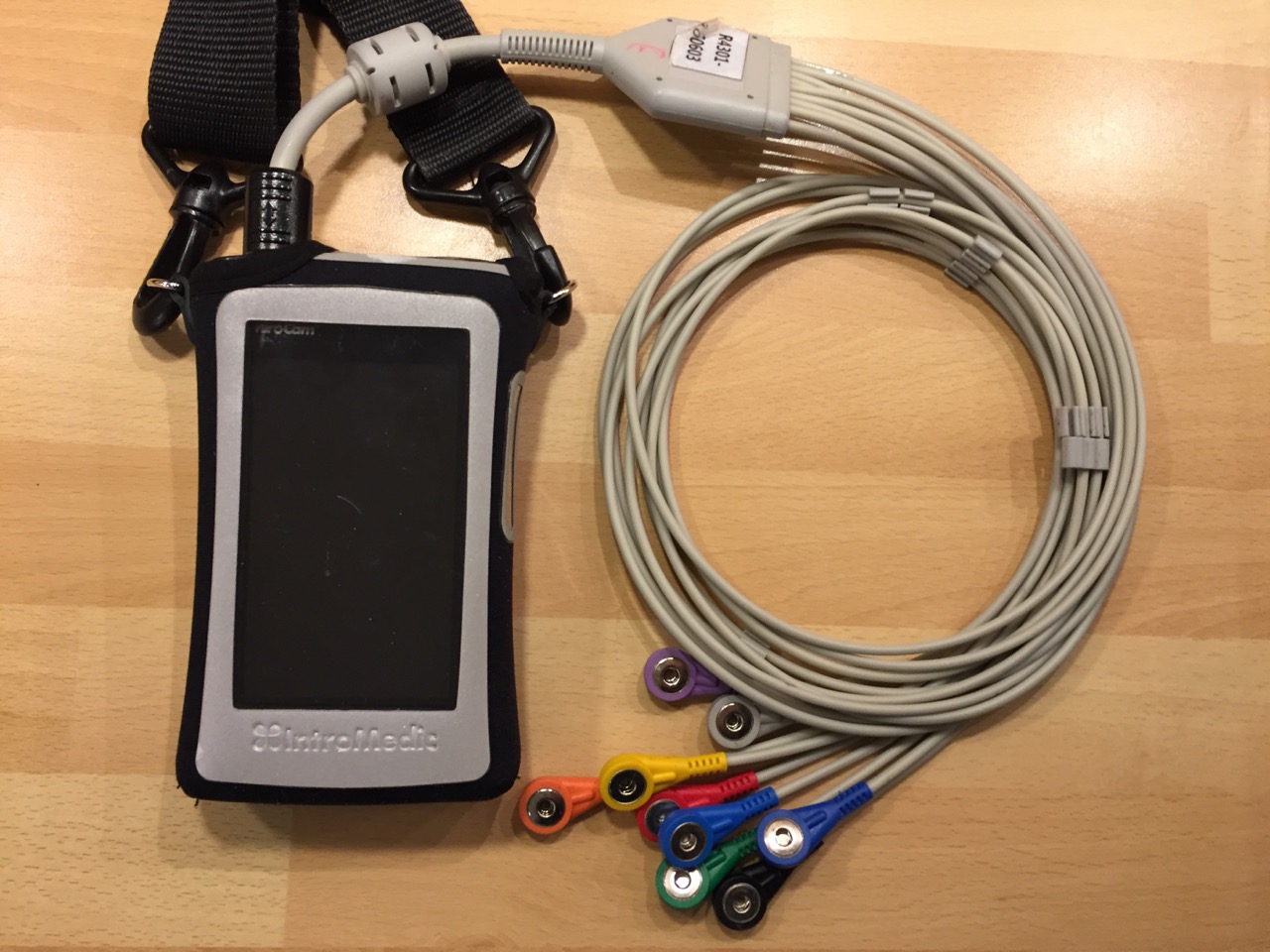
Several different camera systems are on the market, all working on similar principles. There are also different types of capsule for specific tasks. The more advanced ones have higher resolutions & frame rates and some communicate with the recorder unit wirelessly, without the need for sensors. In this instance the MiroCam system was being used with its array of sensors picking up the capsule signal and sending it to the recorder.
The first task was to attach the numbered sensors in the correct positions around the abdomen and connect them to the wiring harness, very similar to an ECG. The harness itself was quite bulky. The nurse then produced the capsule, asked me to hold it between my fingers then pass it in front of the recorder unit. A bleep showed that they had paired. My information had already been entered into the recorder unit with the display showing name, hospital number etc.
How easy was it swallowing the capsule?
The answer, for me, was very easy. One gulp of water and it was on its way. The nurse switched on the live monitoring function and we watched it enter my stomach. To save battery power she then switched it off and I didn’t have the courage to try switching it on again in case I ruined the whole procedure (…and what if I had seen something that, to my eyes, looked wrong? A surefire way of inducing hypochondria).
The unit had a 12 hour battery life and switched itself off automatically after that time had elapsed. I could then remove the sensors and return the recorder unit. The results were due in two weeks time.
When would I be able to eat and drink again? Coffee two hours after swallowing the camera, a light meal after another two hours and then resume normal eating after six hours. You’ll be pleased to know that the camera is not retrieved after the procedure (although there are some types that do rely on the patient “collecting” it and returning it to the hospital for analysis!).
Wearing the receiver unit took me back to having a stoma as it was hanging in the same position as the bag and the adhesive on the sensors gave a similar sensation to that of a stoma backplate.
When the report was available it showed that Crohn’s had re-surfaced in my small bowel in the form of mild to moderate inflammation. This was a disappointment as I had been in drug free remission since 2011. A printed copy of the endoscopy report, in glorious living colour, arrived in the post. I was intrigued by the transit times : 15 minutes to make it through the stomach; 2 hours 52 minutes travelling through the small bowel; and 8 hours 51 minutes in the colon. These were classed as being “within average range”.
Luckily there was a summary report; unluckily there it was in black and white “…with a background of Crohn’s these are in keeping with mild to moderate active disease”. As a result I was started on Vedolizumab.
Video Capsule No.2
In August 2020 I received a call from Endoscopy appointments to arrange for a follow-up VCE to see if the inflammation in my small intestine was still there. I would need the obligatory small bowel MRI first to ensure there were no strictures that could trap the capsule on its journey.
We were in the depth of COVID restrictions and the procedure was considered to be an AGP (Aerosol Generating Procedure) and as a consequence I needed to have a negative COVID result 3 days prior to the hospital visit. It was arranged for a courier to deliver a test kit, wait for me to carry out the test and then return it to GSTT for analysis. It turned out negative.
The endoscopist had been working at GSTT for 15 years but, surprisingly, our paths had never crossed. He explained that the hospital had access to 7 different camera systems and that their prominence as a leading teaching hospital meant that manufacturers were keen to make their systems available. The one they would be using that day was made in Wuhan (yes, THAT Wuhan) and was the first one to include a type of AI which highlighted frames needing particular attention when reviewing. Two representatives from the manufacturer sat in on the procedure to observe it being carried out.
Unlike my previous VCE this capsule transmitted directly to a receiver worn on a belt without the need for sensors. It was a lot more convenient. The output from the camera was displayed on the receiver and also on a laptop.
I asked if it would be possible to examine my oesophageal varices to see if they needed banding. I was hoping to avoid a conventional endoscopy later in the year. Yes, it would be possible by adopting an “oesophageal protocol”, a fancy way of saying you lie down as the camera is swallowed so that the passage through to the stomach is slowed down. Swallowing it whilst lying down was not as difficult as it sounded but even so it only took a few seconds before it entered my stomach.
I lay on a pivoted bed. It was tilted head first, feet first, then left and right so the camera could video all around the walls of my stomach. A patch of inflammation appeared. It would be discussed at the next MDM on Friday. Eventually the camera was allowed to pass into the duodenum and it was time to get back on my feet.
I returned to St.Thomas’ the following day to drop the recorder belt back. Eventually the follow-up letter arrived from the VCE Virtual Clinic. It was good news, very good news. The vedolizumab was doing its job.
Video Capsule No.3
The same again but different : In March 2023 I ended up in our local A&E with internal bleeding. An upper GI endoscopy showed oesophageal varices had regrown despite being OK when checked a few weeks previously. What had caused them to reappear?
A small bowel MRI scan picked up a new clot in my superior mesenteric vein and I went to see a thrombosis consultant. Our discussion boiled down to should I start on blood thinners, something I had declined in the past. Before making the decision he wanted to make sure that I was not bleeding in locations other than my oesophagus hence requesting a VCE.
When the nurse rang to arrange the date for the procedure she said that she would be including sachets of MoviPrep. I remarked that a) I hadn’t had to take prep on the previous occasions and b) if I had to then I would prefer Citrafleet. The instructions arrived together with the Citrafleet.
The preparation was now virtually the same as having a conventional colonoscopy with the same restrictions on the type of medications and the timing of meals during the countdown to procedure day. (Having had the conversation about not having prep I recalled that when I had been through our medicine cupboard I had found a sachet of MoviPrep and assumed it had been sent for some colonoscopy in the dim and distant past. Maybe I hadn’t used it prior to a previous VCE.)
This time the capsule was the two lens version which results in it being larger than the previous ones I had swallowed. That didn’t present a problem but then I have become used to swallowing pills and capsules. Out of curiosity I asked the nurse how they would administer it if someone couldn’t swallow and she replied that it is possible to introduce the capsule with an endoscope!
The set-up was slightly different from before. There was a disposable belt with built-in sensors, fastened with velcro around the waist. A cable connected it to the recorder unit hung over one shoulder. Apart from that the operation was as previously described and at exactly 12 hours from the start the receiver bleeped and switched itself off. I returned the recorder to GSTT the following day.
I mentioned to the nurse that I had a follow-up appointment with the thrombosis consultant in two weeks time. She said that it should be possible to have, at least, a preliminary run through by then but you have to remember there are nearly 100,000 frames produced.
…and then I had a short wait until talking to the thrombosis consultant and deciding if I should start taking blood thinners. By the time of the tele appointment with him the VCE report was available. We covered a lot ground, probably too much to take in to be honest. My case had been discussed at the Thrombosis Radiology MDM and the decision was to not start anti-coagulation. I was quite happy not to be taking even more medication!
February 2025 saw a fellow Crohn’s patient, Rachel @bottomlineibd, and myself launch a new podcast where we will be looking at some of the aspects of living with and treating IBD.
We had originally intended to make an initial 8 episodes but we’re already up to twelve and there are more in the pipeline. The list of current episodes are shown below.
The podcast is available on Spotify, Apple or Amazon. We are currently planning future episodes on – diet & nutrition, surgery, brain/gut axis, bile acid malabsorption – amongst others.
A few years ago, before COVID, a dozen or so Crohn’s patients gathered in a room at Bowel and Cancer Research HQ (now BRUK) with the task of brainstorming the issues and costs that a patient with Crohn’s can be confronted with.
It was part of the process helping a start-up medical company, Motilent, that the charity was providing PPI input to. The aim was partly to show that the early diagnosis of the disease and better monitoring of the effectiveness of treatment would not only provide cost savings to the NHS (or other healthcare provider) but also to the patients themselves.
It was the first time I had been seated around a table with so many fellow patients. Everyone quickly overcame any nerves they may have had and we had a lively, open & honest discussion on the challenges we all faced. (I even learnt what a PICC line was!)
We then split ourselves into sub-groups and brainstormed around a simple diagram that I had produced to prompt our discussions.
When we had completed the exercise I compiled the results and turned them into the mindmap shown below. There are links to download the chart as either pdf or jpg.
This is not exhaustive and please bear in mind this was produced several years ago and some of the detailed items may have changed – for instance wi-fi being available in many situations which opens up in-patients’ choices for entertainment rather than paying for use of overbed screens. – but overall the headlines remain the same.
I think we were all surprised at just how many things we now experienced having been diagnosed with Crohn’s Disease. This is, no doubt, true of many chronic conditions.
I did a very quick calculation around having my ileostomy taking into account time spent on attending OP appointments, procedures, recovery, time off of work etc. In broad terms 8% of my time was taken up with managing my health!
It may be stating the obvious that anyone can end up in A&E but for those of us with chronic conditions, or advancing years, or both, the odds escalate. It’s clearly a stressful time regardless of whether you are the patient or simply accompanying them. News reports of long delays for emergency ambulances and extended waits to gain access to A&E itself make the prospects of a visit even more uncertain.
In the last 13 years I have been an A&E patient five times and have accompanied elderly parents on several other occasions. Over that period I’ve had a chance to see how things have changed and adapt my coping strategy accordingly. (Maybe you could give me some of your own ideas or feedback via @crohnoid.bsky.social or @crohnoid [Twitter] on your thoughts.)
My first two trips were after calling 999 and on both occasions the ambulance arrived within 8 minutes. Yes 8 minutes! Coincidentally it was the same crew each time. The first call (2011) was due to my stoma bag filling, quite rapidly, with blood. The second time (2012) involved the red stuff again but this time I had vomited it and that time I had the added excitement of the siren and blue lights. I’ve written about the incidents in my book.
My wife came with me in the ambulance each time. The main lesson we learnt was that, once you’ve been processed through triage, communication is the biggest issue. With a large number of patients being treated it is simply not possible for each one to be given an update every 5 minutes. If a real emergency is brought in then the doctors and nurses are diverted to treat them. You have to wait until someone approaches you to move to the next stage of your treatment.
I found that having my wife with me made me more stressed! Whilst it was great to have her company I know how much she dislikes hospitals. I ended up worrying about how she was coping with the situation as well as what was happening to me. Double the stress, and as we went further into the night it became a question of what point should she call it a day (night) and make her way home.
In 2010/11 I had spent several weeks in a major London hospital so had become relaxed about being in that environment, having cannulas inserted and all the other checks and indignities that one undergoes. Being in London had made visiting difficult because of the distance from home so I became used to spending extended periods on my own. It has subsequently made it easier to cope but I can understand why it is difficult for those new to the experience.
On my third visit (2017) I had turned yellow (jaundice) and my GP sent me off to A&E. No need for an ambulance this time so I arranged a lift once I had packed an overnight bag, had some lunch and walked into hospital unaccompanied.
Having booked in at reception I was taken to see the triage nurse and then returned to the waiting area. At this point previous experience taught me it was into the unknown and the indeterminate waiting would start. Rather than looking at my watch every two minutes or trying to catch a nurse’s eye, each time they passed by, I decided to set a finite time, in this case one hour, at which, if I had not moved on to the next stage of treatment, I would go to the nurses’ station and ask what was happening. This structured approach seemed to really help.
To pass the time I read a book although it was not always easy to concentrate with all the hustle and bustle going on around one. I managed to keep relatively relaxed. In the end I was moved to a bed in the Medical Assessment Unit, a small ward attached to A&E and I stayed there until I had been seen by a consultant and discharged the next morning. I felt I had managed my stress well, for the most part.
My fourth trip to A&E was in March 2023 after experiencing malaena. I knew that the service level had been considerably degraded due to the lack of resources, staff and onward bed blocking. I was convinced that my previous “set time limits” strategy would not work this time. I packed my bag, said goodbye to my wife and then set off for A&E with some trepidation.
Ever since starting a patient’s blog in 2010 I have found that the creative writing process has been very cathartic. The “reporting” aspect has allowed me to be almost at arm’s length and to view my treatment as if I am a third party, detached. I wondered if treating this latest experience as an “opportunity to witness and report the situation at first hand” would help pass the time and keep stress levels down
I decided to regularly Tweet my progress through the system and illustrate with photographs where possible. A distinct advantage of using SoMe to post updates is that you get feedback from others and it helps to feel that you’re not alone through the ordeal. Even in the wee small hours there is usually someone awake that understands your predicament, has probably been there themselves and responds. There is also the discipline of getting your message across in the limited number of characters.
I decided to copy some of the Tweets to our local MP, Claire Coutinho (East Surrey), so that she was aware of what was happening under her government’s 13 year watch. I didn’t get any response, of course.
The experience was considerably worse than before and I ended up on a bed in one of the A&E corridors for 14 hours before being sent for an endoscopy and then moved to a ward. I was one of many patients waiting in the corridors.
Again I found that by having a “strategy” I could cope with the mind numbingly boring periods when nothing seemed to be happening. It helped that I was fairly sure what the consultant would find when she scoped me and what the treatment would be. Having been through the same issue before I also knew what the aftercare should be and was able to use this to argue for my discharge from hospital sooner rather than later. As I said to the consultant on her ward round – “being in hospital is doing my head in. My recovery will be a lot quicker at home”.
My last visit in December 2023 was quite a different experience from before. I had turned yellow (again) but not too deep a shade. I managed to get an appointment with my GP and told him that I really didn’t want to end up in A&E. He was sceptical. He would make a call to the hospital and ask their advice. They advised him to send me to A&E with a letter explaining the situation.
Off I went to East Surrey hospital with my GP’s letter in my hand. When I checked into A&E reception I was directed straight to the Surgical Assessment Unit with no need to go through triage or spend hours in the general waiting area. That taught me the benefit of having that GP letter rather than just turning up.
Unfortunately our GP surgery has now implemented an online triage system before you can even get a doctor’s appointment. I’m guessing that if I turn yellow again they will send me directly to A&E without the benefit of a GP letter. Not a prospect I’m looking forward to.
Each time I came away from East Surrey Hospital I had nothing but sympathy for the NHS doctors and nurses trying to deliver a first class service without the resources they need. I cannot see the situation improving until the care sector is sorted out and patients can be discharged when they are medically ready rather than when they can be found a space in a care home.
When I was looking for a book title and a name for my rejuvenated blog I wanted something slightly “off the wall”. Whilst I was writing the chapter about surgery looming I came across the consultant’s explanation of the CT scan he had in front of him. “It looks like you’ve got an octopus in there.” That set my imagination running and I pictured the scene in theatre where the surgical team had “released the octopus”, cut out the offending bit and then wrestled the remainder back, safely, into my abdomen.
Search for title over and seed of idea for book cover sewn.
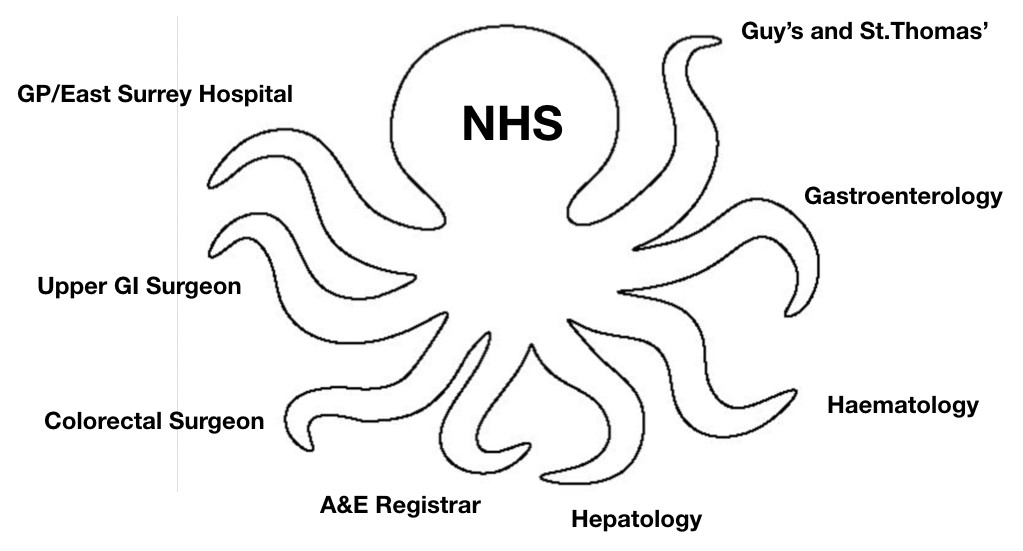
As I neared the end of writing it occurred to me that there was a second octopus to be wrestled. It’s potentially a problem for all of us that suffer from chronic illnesses, namely, managing our route through the multiple tentacles of the NHS system with multiple consultants, procedures, specialities and clinics. Add to this the lack of a universal patient record system that can be accessed in different hospitals and it is apparent it’s not necessarily a simple process.
Life was simple when being treated by one gastro team at one hospital. It wasn’t until 2010 that another hospital entered the equation as my local hospital were unable to cope with the complexity of the forthcoming surgery and referred me to St.Thomas’.
This calls for a diagram –
My Personal Octopus
Some “tentacles” act in a co-ordinated manner; others seem to be a law unto themselves. Some tentacles communicate well with the others, unaided; others need a helping hand.
For example, if you’re booked to go for a procedure, let’s say an MRI scan, then it makes sense that your next gastro appointment is after the radiologist has written the follow-up report. Similarly, if you’ve had biopsies taken during a colonoscopy, you want the results to be available before you meet your gastro. This is not rocket science but if not co-ordinated then you simply end up wasting valuable appointments, consultant’s time and, just as importantly, your own time.
In the past I’ve let the system take its course but with mixed results so now I like to give it a helping hand. This is getting more difficult with the apparent demise of the dedicated medical secretary. For several years, when the frequency outpatients appointments and procedures had reached its height, I had the pleasure of dealing with a truly exceptional one. Let’s call her Sally. Any issues would be quickly resolved by a simple exchange of emails. Sadly she left the NHS.
Nowadays I contact my consultant directly, but sparingly. I don’t particularly like doing it as I know he is already exceptionally busy. I can justify this approach to myself as in the long run time/resources will be saved by avoiding abortive appointments. I suppose you could now say that I am “massaging the octopus” rather than an all-out Greco-Roman grapple.
…and now I’ve identified a third “octopus”. Unless you’ve lived with a chronic illness it must be near impossible to grasp all the issues that have to be dealt with. Is Crohn’s worse than any other disease with those regular colonoscopies and a 70% chance of surgery? A number of Crohn’s patients came together for a brainstorming session to document their experiences. The resultant mindmap, showing the extent of the disruption to one’s life, resembles a multi-tentacled octopus and is as difficut to wrestle into submission!
If you have read some of my previous posts or followed me on Twitter it is likely you have seen my “jigsaw” diagram in its various incarnations. I drew it, initially, to try and understand the relationships/causes between the various conditions I have ended up with and to make sense of 30+ years of medical records which I obtained, in one go, from three Health Authorities. The notes were a mixture of handwritten ward notes, typed letters and a raft of pdfs on CDs. I was amazed that they stretched all the way back to 1977.
Medical Records – from 1978 onwards
The diagram started out very simply.
Crohn’s Jigsaw – Version 1
It then dawned on me that it would a good way of showing a new doctor or surgeon the complexity of my case on just a single page. This second illustration is the first development of the early version.
Early development of first diagram
I attached this more developed version to a Tweet during a #patientchat to illustrate how I like to communicate. The very positive response that I received from both patients and doctors was very gratifying. There were a number of requests for the template I used. I have therefore removed the text that was specific to my case and saved the file in both the original Keynote format and a Powerpoint format.
If you click on the links at the bottom of this post you will be able to download the appropriate file. Please feel free to use them however you wish. I hope you find it useful and would be grateful if you could credit me if you use it.
This template should get you started on mapping your medical history
Here’s the version of the diagram taking the story up to April 2021
…and here’s the most up-to-date version, taking the story up to October 2023. You will see that it has had to undergo some redrawing to fit everything in and I’m running out of space!
…and at one point someone set me the challenge of making an interactive version. Taking the initial, simple diagram I added more “nodes” that when clicked would open up the relevant documents or test results.
The link below will take you to a web based version, although it has not been updated for a while. It was not too difficult to set up but needed a knowledge of “mapping”. The most time consuming part was redacting personal details from the documents.
…and then taking it to its logical conclusion, and with thanks to the example set by @MightyCasey, who sadly passed away earlier in 2023, here’s a temporary QR tattoo. It does work. Try pointing your smartphone at it.
…and finally I decided to see how easy it would be to animate the Jigsaw to tell the story in 90 seconds. (This is not based on the latest version). Here’s the link :
Over the years I have undergone many different tests but the one that had eluded me to date was the Video Capsule Endoscopy (VCE). Maybe that’s the wrong to put it. Might be better to say that “so far I hadn’t needed one”.
So what changed? The last time I saw my gastro we discussed the apparent conflict between my feeling fit and well (good QOL), clear colonoscopies & biopsies but test results suggesting the opposite – calprotectin = 1300 ; Hb = 11.0 ; gradual weightloss >15kg. We had discussed this before. He had even asked a colleague to carry out a second colonoscopy in case he had missed something. Both of them were stumped so we agreed to park it. I thought now was the time to ask for it to be investigated further. The only part of my digestive tract that hadn’t been seen through a lens was the small bowel between duodenum and the point where my large and small intestines had been rejoined. He agreed.
We had previously discussed using a self-propelling endoscope but a “pill cam” sounded a less daunting solution. The concern about using a capsule was the risk of it becoming stuck at a narrowing. A radiologist would be asked to review my last MRI scan for strictures before the endoscopy was ordered. The cost of the capsule endoscopy procedure to the NHS is approx. £500.
All must have been well as I got a call from Endoscopy Appointments to agree a suitable date for the procedure. A couple of days later the instructions arrived in the post. Very similar to having a colonoscopy but with none of the dreaded prep solution needed. The leaflet also listed the medications that would have to be put on hold. These included stopping iron tablets and Loperamide 7 days out. Iron tablets – no problem, but Loperamide – that would be the one instruction I wouldn’t be following. The thought of taking a trip to London having not taken Loperamide for 7 days was not even worth considering and would have put in jeopardy attending the Big Bowel Event at the Barbican on 16th November.
Monday 19th November 2018 – GSTT Endoscopy Department
After the glorious weather over the weekend it was a disappointment to arrive in London on a dull, rainy day. The walk to the hospital took me past a number of foodstalls that simply reminded me that I hadn’t eaten since 8:30 the previous morning or drunk anything since 22:00.
One of the food stalls that have sprung up along the South Bank
I arrived at St.Thomas’ Hospital and, after a few minutes’ wait, was collected by the specialist nurse. She asked the usual questions :
“When did you last eat?” “8:30 yesterday”
“When did you stop taking iron tablets?” “7 days ago. Why is it so far in advance?” “They blacken the walls of the intestine and can give patients constipation”
I explained that I hadn’t stopped taking Loperamide as, for someone who relies on it every day, any thought of stopping for 7 days was a definite non-starter.
“What other medications are you on” I went through the list
She outlined the procedure and I was able to ask the questions. The main one was “can the capsule be used to judge the condition of esophageal varices? If it can then should I cancel my conventional Upper GI endoscopy booked for the week before Christmas?”. She explained that a capsule can be used to look at varices but it would need to be a different type from the one I would be swallowing today.
She then ran through the risks of the procedure. The main one being the capsule becoming stuck and the possible means required to extract it, the worst scenario being surgery. I signed the consent form.
There are several different makes of capsule system available which all work on similar principles. There are also different types of capsule for specific tasks. There is even one with a camera at both ends.
The more advanced ones have higher resolutions & frame rates and some communicate with the recorder unit wirelessly, without the need for sensors. St.Thomas’ employ the MiroCam system which uses an array of sensors to pick up the signal from the capsule and send it to the recorder. (It’s the same unit that the BBC used for the live endoscopy that they broadcast as part of their “Guts: The Strange and Mysterious World of the Human Stomach” in 2012.)
MiroCam receiver and sensor array
The first task was to attach the numbered sensors in the correct positions around the abdomen. I can see why wireless communication is the future. (I wouldn’t normally post a selfie of my abdomen, in the interests of good taste, but to illustrate…..)
It’s not until you see a photo of your abdomen you realise the marks that have been left by surgery, laparoscopic not keyhole
Once they were in position the nurse produced the capsule and asked me to hold it between my fingers then pass it in front of the recorder unit. A bleep showed that they were now paired. As she had already input my information into the unit the display showed my name, hospital number etc.
The capsule – measuring 25mm long x 11mm dia.
It was time to see how easy swallowing a capsule would be. The answer – very easy. At 11:40 I took one gulp of water and it was on its way. The nurse switched on the live monitoring function and we watched it enter my stomach. To save battery power she then switched it off and I didn’t have the courage to try it myself in case I ruined the whole procedure. (…and what if I had seen something that, to my eyes, looked wrong? A surefire way of inducing stress)
As the unit has a 12 hour battery life she said the unit would switch off at 23:40 and I could then remove the sensors. The recorder unit would then need to be returned to St.Thomas’. I explained I was not available the following day so we agreed that I would take it back on Wednesday. Two weeks later the results should be available. When would I be able to eat and drink again? Coffee two hours after swallowing the camera and then a light meal after another two hours.
If it had been decent weather I would have set off on a long walk around London, as light exercise helps the transit of the capsule, but I decided I would rather get home in the warm. I took a short walk to College Green (the area outside the front of the Houses of Parliament) to see if there was a media scrum due to some new development with Brexit but there wasn’t so jumped on the Tube to Blackfriars and took the train home.
From Platform 1 at Blackfriars there’s a good view of the City and the new buildings going up
True to the nurse’s word the unit switched itself off at precisely 12 hours from the start of the procedure and I was able to peel off the sensors with remarkably little pain. The camera is not retrieved after the procedure (although there are some types that do rely on the patient “collecting” it and returning it to the hospital for analysis).
Wearing the receiver unit took me back to having a stoma as it was hanging in the same position as the bag and the adhesive on the sensors gave a similar sensation to that of the stoma backplate.
Partial Update
The analysis of the video was due to take 2 weeks from handing the recorder unit back but nothing was forthcoming. I contacted my gastro consultant who said he would chase it up but after 4 weeks still nothing. I knew I would be visiting the Endoscopy Dept. again on 18th December, for my annual Upper GI scope (looking for esophageal varices related to portal vein thrombosis) so I would ask then.
The endoscopy was being carried out by the head of the Gastro Dept. so I asked him whether he could find my video results on the system. He went off to check the status. By the time he returned I had been prepared for the scope – xylocaine spray (burnt bananas) to back of throat; mouthguard in position; Fentanyl injected. I was unable to speak. Luckily they had held off with the Midazolam so I was, at least, still conscious!
He told me that the video was being checked now but he had seen the first half of it and appeared to show Crohn’s in my small intestine. A nice Christmas present! I would have to await the full analysis before discussing the way forward. I emailed my gastro consultant to tell him the news. He replied that he would keep an eye out for the report.
…and with that the Midazolam was injected….zzzzz
When Will It Be Resolved?
The report took a long time to finally emerge and in another email my gastro said that it did indeed show that Crohn’s had re-surfaced in my small bowel in the form of mild to moderate inflammation. This was a disappointment as I had been in remission since 2011. An appointment has been arranged for 15th April to discuss the treatment options. If feasible I would favour the “do nothing” option. My thoughts on the end of remission and the questions I have for my gastro are in a separate post (opens in a new window) – https://www.wrestlingtheoctopus.com/call-my-bluff/
The Report Finally Arrives
In mid-March a printed copy of the endoscopy report, in glorious living colour, arrived in the post. Whilst I found it fascinating I struggled to understand exactly what the images were showing.
I was intrigued by the transit times : 15 minutes to make it through the stomach; 2 hours 52 minutes travelling through the small bowel; and 8 hours 51 minutes in the colon. These were classed as being “within average range”.
Luckily there was a summary report; unluckily there it was in black and white “…with a background of Crohn’s these are in keeping with mild to moderate active disease“.
Capsule Endoscopy Report – from esophagus to ileo-caecal valve
I had a colonoscopy a few days ago, the first one in five years. I’d forgotten the detail of what was involved probably because, in the meantime, I’ve had seven gastroscopies which do not require any preparation but are done under sedation.
If you’re reading this then I’m guessing you’ve either had a colonoscopy and want to know if your experience was similar to mine or you’re about to have one and are looking for some information on what it is like from a patient’s perspective.
First, the bad news. A couple of years ago I ran a quick poll on Facebook asking which of the tests IBD patients rated as the worst. Of the 700 responses almost 70% chose a colonoscopy. For the remainder it was mainly the dislike of having an MRI scan.
There is no disguising the fact that the colonoscopy is widely despised by patients and I wonder how many, with digestive problems, put off seeing their GP because they do not want to undergo this procedure. Unfortunately there are no alternative ways of taking biopsies in the gut but for some monitoring activities there is light at the end of the tunnel. More of that later.
The colonoscopy experience can be broken down into 4 acts – fasting, preparation, scoping and recovery. How does this work in practice? Let me use my recent experience to illustrate.
Act 1 – Fasting – started with a fibre free diet 3 days out. The following day I was allowed a light breakfast then liquids only until after the procedure. On the last occasion I made myself a mug of Marmite dissolved in hot water. It was disgusting and turns my stomach just thinking about it. Suggested alternatives were Bovril or an OXO cube. I tried a “vegan, beef favoured” OXO cube in hot water and took the first sip with some trepidation. To my surprise, it was very tasty. I have struggled with fasting in the past but this time it was fine.
Act 2 – Preparation – the dreaded purging liquid that many find the worst part of the whole procedure. There are three common brands – KleanPrep, MoviPrep and Citrafleet/Picolax – and they are taken in 2 doses. The most obvious difference is in the amount of liquid you mix up. KleanPrep requires 2 x 2 litres; MoviPrep requires 2 x 1 litre; Citrafleet/Picolax only requires 2 x 150ml.
There are medical reasons for using different types, for instance the ones requiring higher volumes of liquid are less likely to affect your kidney function. Luckily at GSTT the standard issue is Citrafleet. At 4pm I swallowed 4 senna tablets and an hour later downed the first 150ml of prep. Previously it had taken effect very quickly and I had not strayed far from the bathroom. This time the hours passed before….well you can guess!
Five years ago you would take the second dose of prep later that evening but then the instructions changed to taking it on the day of the procedure. I am very sceptical about this. I have a 90 minute journey from home to hospital, mostly on public transport, and the last thing I want is to still have anything left in my gut. As a compromise I got up very early in the morning and downed the second dose ready for the procedure that afternoon. Had my appointment been in the morning then I would have taken the dose late the previous day and put up with a disturbed night.
Let’s talk about sedation for a moment…
Sedation is commonly a cocktail of midazolam and fentanyl. I’ve heard the former described as the “vallium” of the mixture and it has memory suppressing qualities similar to rohypnol; fentanyl is the painkiller but also enhances the effect of the midazolam. The best way to describe the effect is, to borrow from Pink Floyd, you are comfortably numb but sufficiently conscious to respond to the endoscopist’s requests to adjust your body position as required.
Sedation has implications. If you choose that option you will need someone to escort you home and you are not allowed to drive for 24 hours as your insurance would be invalid.
I had looked back at old colonoscopy reports. They all showed sedation and yet I remembered coming home without supervision on at least one occasion. Putting two and two together I concluded that I would not need an escort so didn’t organise one. When I re-read the appointment instructions it clearly stated no escort, no sedation. That left me in a quandary. The options – find an escort or have no sedation or cancel the procedure. I decided to ask the IBD community on Twitter if no sedation was an option I should consider. I was inundated with responses ranging from “of course you need it” to “you’ll be fine without it”.
In another poll, this time on Twitter, patients were asked about their sedation preferences. Nearly 500 responded of which 80% chose sedation; 9% no sedation; 7% said it depended upon their disease activity; and the final 4% said it depended who was carrying out the procedure.
I Tweeted that I had not managed to organise an escort, half hoping that someone might be able to help but I thought it was probably a forlorn hope. I was delighted to get many replies from patients and non-patients saying that if they were based in London they would help. Even more heartening two people actually offered to act as my escort. The wonder of social media! I made contact with one of those who had replied and she was very happy to assist.
The week before the colonoscopy I happened to have a tele-appointment with my gastro consultant. He would also be driving the scope. I told him of my dilemma and he said that I would be fine with just “gas and air” (Entonox) and that he would go very carefully. That made my mind up – no sedation and therefore no escort.
On the day of the procedure I set off for London early so that I could take some photos of the River Thames before my own, internal, photo session……
HMS BelfastGuy’s Hospital at London Bridge, next to The Shard
Act 3 – Scoping – having found the Endoscopy Suite, despite the lack of signage, I was greeted by the receptionist. “Hello sweetheart, what’s your name?” Once signed in a nurse showed me to a cubicle and gave me two surgical gowns, some hospital socks and a pair of “modesty” shorts. After running through a checklist he took my blood pressure and I took a COVID LFT. He left me whilst I changed into the hospital clothes. The modesty shorts have an opening at the back. On a previous occasion I had managed to put them on the wrong way round and they had proved to be anything but modest.
At this point, if I had opted for sedation, the nurse would have inserted a cannula (and I would have obeyed the second law of cannulation that you must take a photo and post it on SoMe). A few minutes later my consultant appeared, ran through the potential risks and I signed the consent form. With that completed he led me to the procedure room. The nurses introduced themselves and I lay down on the trolley. One of the nurses showed me how to use the Entonox. It is delivered via a mouthpiece and if you feel any discomfort you take a few deep breaths to mask it.
I rolled over onto my left side and drew my knees up. The monitor was showing my heart rate as 65 bpm. With the camera inserted it was an easy run until the sharp bend (splenic flexure) was reached. That is where the skill of the endoscopist really comes into play. I was asked to roll onto my back. Air is used to inflate the gut and make the passage of the camera easier. Every so often a water spray is deployed to clean the lens or flush any debris that the prep solution didn’t dislodge.
Being wide awake I was able to watch the whole procedure and ask what we were seeing. On screen there is a small “satnav” window that shows the 3D position of the endoscope. There was some very mild inflammation in the colon but “nothing that needed treating or to worry about and your last calprotectin was 37. I’ll take a few biopsies on the way out”.
I used my time to ask questions. One in particular I was keen to know the answer to. When I had a stoma I had been surprised that this thing, part of my intestine, that was sticking through my abdominal wall, was impervious to touch. It had been explained to me that the gut has no nerves so I asked if this was true. Yes, it was. If there were nerves in the gut you would feel every piece of food passing through it. That made sense. The question I should have asked, of course, was how does the inflammation square with the low calprotectin score.
The camera made its way ever onwards. There were a few difficult manoeuvres that required withdrawing a few centimetres and then re-orientating it with the assistance of the 3D image. The camera reached just beyond my anastomosis – the surgical join between my small and large intestines – made easier as my ileocaecal valve and terminal ileum were removed in 2010.
“You can tell we’ve now entered the small intestine as the walls have a different structure and that is how food is absorbed.”
Time for the camera to be withdrawn and the biopsies taken. I had never considered how the biopsy samples got from the gut into phials ready to go to the lab. Being fully awake allowed me to watch the process. The endoscope tube has a cavity through it that allows a separate instrument, with a pair of small forceps on the end, to be pushed out beyond the scope. The tool takes a biopsy from the gut wall, directed by the endoscopist, and then one of the assistants withdraws the tool and retrieves the sample. The tool is then re-introduced through the endoscope and the process repeated.
Watching the grab collecting samples is slightly disconcerting as you expect to feel it and there is a small trickle of blood at each location but no nerves, no feelings. After a dozen biopsies had been taken the procedure was over. I had hardly used the Entonox and will choose the no sedation option for future colonoscopies. The results would be ready in two weeks time. My consultant asked me to email him at that point. I wonder if the results will explain my calprotectin question?
My Twitter conversation about the advisability of not having sedation had reached him and he had done some research. Looking through the records he found that I had a colonoscopy in 2015 without sedation. That explained why I recalled not needing an escort.
The final discussion before leaving the procedure room was about alternatives to having a colonoscopy. My consultant said that when biopsies are not needed then ultrasound was looking promising and that its use was taught as standard in some countries but not UK. Let’s hope that changes.
Act 4 – Recovery – if you have had sedation then you will be taken in to a recovery area until you have regained full consciousness and have changed out of the hospital clothes. Your escort will be told you are ready for collection. Before you leave the cannula is removed and you will be given a copy of the colonoscopy report. My report showed that the prep was “excellent”. It concluded with a series of “IBD Scores”. The only one that wasn’t zero was the SES-CD (Simple Endoscopic Score for Crohn’s Disease). The score was 3 which equates to “mild endoscopic activity” and is the lowest of the scores after “remission”.
There may be after effects, one of the commonest being discomfort caused by the inflation of the gut. I didn’t notice any of this. Another issue is that the prep has decimated your gut microbiome and this takes time to re-establish. After a week I’m still not convinced is has returned to normal. I have been taking a pro-biotic yogurt to try and help the process along.
The colonoscopy experience was over.
UPDATE: I contacted my consultant for the biopsy results. “Biopsies of colon totally normal… consistent with calprotectin…..”
The next performance was a gastroscopy (an Upper GI endoscopy) one week later but I can’t tell you a lot about that as I was away with the fairies. Thank you midazolam and fentanyl……and my escort.
Final thoughts – for those about to have their first colonoscopy I would suggest that you arrange an escort and opt for sedation. It can make the procedure a lot less stressful. If you subsequently become an “old hand” at scoping you may want to review your options.
I think we have all felt embarrassed about where they are going to stick that camera but I try to remember that the Endoscopy team will have seen it all before. It is a routine procedure that they carry out multiple times a day. When it is your turn I hope it all goes well.
I had been meaning to update this for a while. I compiled my list of ten things I learned would make life easier during my more recent stays in hospital (UK NHS – 2 bowel operations; 2 emergency admissions (one with a 2 weeks recovery stay). I wanted to pass them on in case it helps to improve your “end user” or “patient” experience. I thought I’d ask some patients if they could add o my initial list so I posted the question on a Crohn’s Forum. Thank you – xxSophiex, IHurt, CDJ, UnXmas, acc929, SickofCrohns for your additions.
Here’s the updated version which has now grown from 10 to 18. I’m not suggesting you take all the physical items listed below with you in one go. I’d go for a phased introduction as your recovery progresses.
One possible risk to bear in mind is not being able to keep your expensive technology securely whilst you’re in hospital. The wards I’ve been on have discouraged the bringing of valuables into hospital for this reason but realistically everyone will want their mobile phone with them. The ideal solution would be for each bed to have a patient lockable drawer/cupboard but I’ve never seen one in the NHS. There may be a ward safe that you can ask for valuables to be stored whilst you are in theatre and recovery.
No.1 MOBILE PHONE – it goes without saying that you will have your phone with you but not so long ago you weren’t allowed to use them on the wards. There may still be restrictions in certain sensitive areas. Don’t forget your charger, preferably with a long lead in case the mains sockets are halfway up the wall.
No.2 HEADPHONES – there are lots of times when you really want to be able to drown out the surrounding ward noise. I prefer to have two pairs of headphones with me – in ear and over ear. Over ear will give you the best isolation from the ward noises but you can’t comfortably lie on one side with them on and your ears tend to get hot! The in-ear may not be as good for keeping out external sounds but you have more choice in your sleeping position. (A good pair of noise cancelling ones would be a good idea).
No.3 EYE MASK – like the ones you have for air travel. It’s very rare to have all the lights off in a ward and even if they are, the nurses will be frequently checking on the more poorly patients so the over bed spotlights will be going on and off throughout the night. That’s where the mask comes into its own.
I haven’t actually tried a mask so have found the best time for dosing is during the mid-morning lull. That’s the bit between the doctors doing their ward round; the beds being made ward round ; having a shower and lunch being served.
No.4 SHOWER GEL/SHAMPOO – sometimes these are available in the hospital but there’s nothing like having your own, favourite brand to keep you in touch with home. It’s said that smell is the strongest sense for recalling memories. There is one particular shower gel that I bought ready to go into St.Thomas’ and I used that “flavour” for several years afterwards. Every time I caught that fragrance it would immediately transport me back to the first shower I had post operation – a happy time despite the surroundings.
No.5 SOCIAL MEDIA – I have found the support received on SoMe when one is isolated in hospital is a great comfort. If you wake up in the middle of the night, in pain and can’t get back to sleep there is usually someone out there who will respond with positive messages.
No.6 PYJAMAS AND DRESSING GOWN – the admission instructions may ask you to bring in your night clothes but I have found that pyjamas are usually available anyway. That’s fine if you’re not fussed about the colour. After my reversal operation I was issued with bright orange pyjamas so it looked like I had just escaped from Guantanamo Bay. I try and use NHS pyjamas for a few days after an operation in order to give anything that might be oozing a chance to stop oozing and then it’s into my very stylish M and S ones for the rest of the stay.
The dressing gown is a must. Not only can it give you a bit of extra warmth when sitting about but also covers up that embarrassing gap up the back of your medical gown where you haven’t quite managed to do the tie-ups. (They usualy give you 2 gowns nowadays to address the gapping issue)
No.7 BOOKS AND MAGAZINES – there will be times when you’re not dozing but you really don’t want to warcg more movies or, even worse, daytime TV! A decent book or some magazines, preferably with lots of photos and no difficult text, are a good way to pass the time. I was given a volume of Sherlock Holmes short stories and found that each tale was just the right length to read before needing a rest.
No.8 CASH – This item is a bit of a throwback and was, once upon a time, relevant. I expect everything is contactless nowadays so don’t forget your card.
No.9 MAKE-UP – I’m a bit out of my depth here because I’ve never knowingy worn make-up. I’ll quote directly what acc929 said : “I think this is probably a bit more on the girly end of things, but I’ve found that taking good care of myself (when possible of course) in hospital helps keep my morale up. I think the sicker you look, the sicker you feel, so if you have the energy it’s worth making a little effort. I bring my nice robe so I don’t need to wear the hospital gown, my favourite perfume, and my own shower stuff in little bottles. I bring a tiny bit of make up so that when people visit I don’t need to deal with them telling me how tired I look (I’m in the hospital, duh!) Bottom line, having your own things makes everything feel better.”
No.10 FAVOURITE SNACKS – after an operation or maybe a bad flare-up you may need something to help you get your appetite back. If you have some favourite snacks or chocolate bars etc. pack a few in your bag. Some hospitals have will provide snacks anyway but I don’t know how common it is. The two wards I spent time in at St.Thomas’ always had a good selection freely available. You only had to ask!
No.11 SANITISING WIPES – with all the nasty infections that appear in hospitals nowadays – such as Mrs.A – sanitizing wipes to wipe down any surfaces or objects that you can’t be certain have been throroughly cleaned or disinfected. (May have been superceded by COVID precautions)
No.12 HAND CREAM AND LIP BALM – the atmosphere in the wards is often very dry so creams and balms will help you keep your skin feeling good.
No.13 LISTS – pen and paper – or you could use an app on your phone or tablet. I have always found it useful to write down any questions I want to ask the consultants on their ward rounds. I’ve tried keeping a list in my head but when you are confronted by the consultant and a gaggle of junior doctors, early in the morning, it’s easy for all thoughts to just disappear.
No.14 PAIN – if you start feeling pain or a different pain don’t be brave and keep it to yourself TELL THE NURSE. It may be nothing and you can be given painkillers to help. On the other hand it could be something that needs attention and the sooner that attention starts the better.
No.15 INHIBITIONS – try and lose any inhibitions you may have about discussing the more intimate details of your condition with the medical staff. You may notice something different about your body or what comes out of it. Again it may be nothing or it might need further attention.
No.16 CANNULAS – if you have to have a cannula and, let’s face it, it’s pretty much a certainty, don’t let a doctor put it in. No matter how much practice they claim to have had they are never, ever, as good as an experienced nurse. In the past I have actually said to a doctor ‘”Are you sure you are good at inserting these?”. He assured me that he was but an hour later I had to have it redone as there was insufficient flow through it. This has happened on several occasions so I stand by my “never trust a doctor with a cannula” statement.
I accept that the positioning of the cannula is governed by where a good vein can be found but if at all possible try and avoid having it on the bend of the arm as you will frequently be interrupting the flow when you move your around. The automated pump will start bleeping which will quickly become annoying for both yourself and your fellow patients (and the nurses). If you get a choice of which arm it is put in remember you will have eat meals and manage in the bathroom with it connected. Choose carefully!
No.17 PHARMACISTS – when it’s time to be discharged I can guarantee that you will be ready to go but will then have to wait several hours whilst pharmacy get the correct medications up to the Ward and you can finally leave. If you make friends with pharmacist on their daily ward rounds you can preempt that wait my persuading them to make sure the necessary tablets, in the correct numbers, are in your bedside locker ready for discharge.
If you live near the hospital you may be able to go home and then get someone to return later to pick up your medication.
No.18 SENSE OF HUMOUR/COURTESY – not always easy to keep hold of this when you’re drugged up to the eyeballs, have got tubes coming out of every orifice and your future is uncertain but if you can do your best to keep your sense of humour and treat the doctors, nurses and other patients with courtesy then it will make your stay a lot more bearable. Of course you may be one of those unlucky individuals who has had a humour bypass in which case you should get on well with some of the doctors I’ve met!
That’s the revised list. If I had to choose just one physical item to take in with me it would still be the headphones as they give you the chance of getting some sleep in a noisy environment. The one behaviour I would adopt is a combination of the above but can be summed up as “acceptance that a hospital regime will probably be completely alien to your usual way of life but you do not need to lose your sense of dignity, humour or courtesy”. If you feel any of these are being compromised – complain.































{kind=link}